|
Friday Links
via Blogger http://jeanxrussell.blogspot.com/2021/10/friday-links.html October 02, 2021 at 04:45PM
0 Comments
International Reference Pricing: Cross-country comparison
The price of pharmaceuticals are much higher in the U.S. than in other countries. Some policymakers have claimed that international reference pricing could be used to lower the cost of drugs in the U.S. For instance, the Lower Drug Costs Now Act (HR 3) proposed setting the maximum negotiated price Medicare would pay at 120% of the basket average of other developed countries. Further, these prices would be made available to the commercial health plans as well. International reference pricing, however, has a long history and has been fairly widely adopted in a number of European countries. The exact mechanism through which international reference pricing is implemented, however, varies across countries. A paper by Rand and Kesselheim (2021) conducts a landscape analysis of how different countries (and US proposals) have or have not used international reference prices to inform drug pricing. A helpful summary table from that paper is reproduced below. 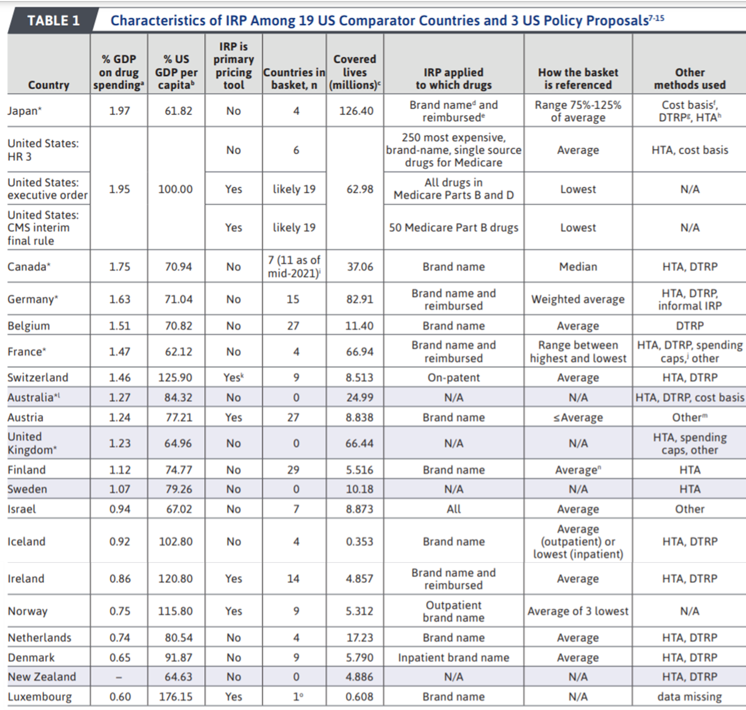
via Blogger http://jeanxrussell.blogspot.com/2021/09/international-reference-pricing-cross.html October 01, 2021 at 02:45PM
Digital health in Europe: Before and after COVID
An interesting report from the European Observatory on Health Systems and Policies examined the “Use of digital health tools in Europe: before, during and after COVID-19“. Digital health is important not only because the technologies facilitate communication and disease monitoring, but also the technologies facilitate the creation of data that can be used to better improve health. Examples of digital health technologies include:
One key item of note was that use of digital health technologies prior to COVID-19 was highly heterogeneous across European countries.
The figure below highlights the variability in uptake of digital health prior to the COVID-19 pandemic. 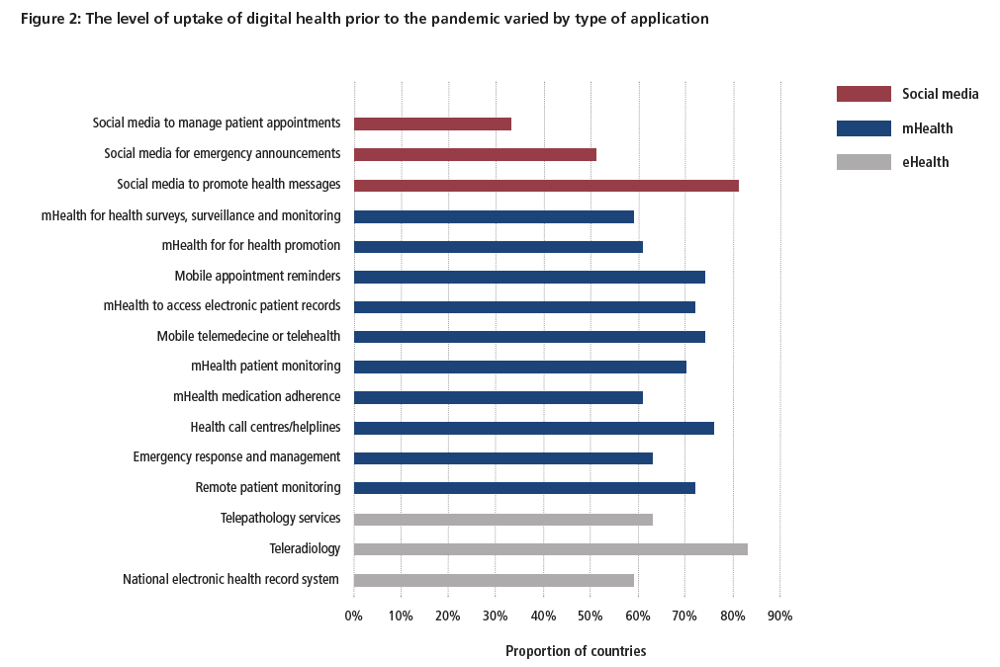
Note that many of the obstacles related to implementing digital health solutions were not technical, but rather systems based. Largely these barriers are legal and financial.
Gaps in the current digital health regulatory framework are found across European countries:
Provider training on the use of digital health tools is also important, but the degree to which providers have been trained in the use of digital health tools is also highly heterogeneous across countries. While digital health is often beneficial to the average patient, its impact on health disparities is unclear.
Digital health was used during COVID-19 in a variety of ways. Most know that digital health was used for telemedicine, appointment scheduling, contact tracing, symptom reporting, vaccine adverse event monitoring, immunity certification (i.e., vaccine passports), hospital capacity management and in many other ways. However, few may be aware that digital technologies were also used in Ukraine to enforce quarantine at home mandates.
Despite the progress made to date, future research is needed to more completely capture evidence on digital health’s cost and benefits of to society. Via Dental Tips http://www.rssmix.com/via Blogger http://jeanxrussell.blogspot.com/2021/09/digital-health-in-europe-before-and.html September 30, 2021 at 11:45AM
How happy are you?
This question seems simple, but answering the key factors that impact your happiness is complex. Is happiness based on your personal situation (e.g., family, job, income, health) measured in an absolute sense or relative to others? If measured in a relative sense, what reference point is used? One approach to measuring your life satisfaction is to use Multiple Discrepancies Theory (MDT), an approach developed in Michalos 1985.
Certainly some previous research has examined absolute versus relative differences but the time component of MDT is interesting. There is some evidence that the timing of well-being may make a difference. Consider the case of the impact of changes in income on happiness.
A recent study by Neumann-Böhme et al. (2021) aims to identify if these reference points make a difference and how differences in income and health affect life satisfaction. They surveyed over 500 people in the Netherlands examining the relationship between income, health (measured using EQ-5D) and life satisfaction (measured using the Satisfaction with Life Scale (SWLS)). Based on this approach, they found:
The findings are interesting in that not only does life satisfaction depend on health and income, but these quantities are valued relative to multiple internal, external and temporal reference points. Source:
via Blogger http://jeanxrussell.blogspot.com/2021/09/how-happy-are-you.html September 29, 2021 at 11:45AM
Quantifying patient administrative burden
Previously, I wrote about how the US healthcare system imposes $90 billion of costs on physicians related to drug utilization management. According to a study by Kyle and Frakt (2021), the U.S. healthcare system also imposes a significant burden on patients as well. The authors use the 2019 Health Reform Monitoring Survey (HRMS) to answer this question. Administrative burden is measured as having to complete one of the following tasks in the past 12 months: scheduling, obtaining information, prior authorizations, resolving billing issues, and resolving premium problem. Based on the responses from 4,155 individuals, the authors find that:
As anyone who has needed medical care recently can attest, we certainly can make the U.S. healthcare system more patient-friendly. Via Dental Tips http://www.rssmix.com/via Blogger http://jeanxrussell.blogspot.com/2021/09/quantifying-patient-administrative.html September 28, 2021 at 10:45AM
Your weekend reading list
via Blogger http://jeanxrussell.blogspot.com/2021/09/your-weekend-reading-list.html September 25, 2021 at 03:45AM
Barriers to biosimilar adoption
When typical drugs lose their period of exclusivity, new generic competitors arrive on the market with drastically lower prices. As patients switch from brand to generic drugs, the price of treatments declines. For biologic drugs, biosimilar uptake, however, is significantly less. In part, this is because biosimilars are difficult to manufacture so the price differences between biologics and biosimilars are typically smaller than the differences between brand and generic pills. Nevertheless, a study by Mulcahy, Hlavka and Case (2018) found that biosimilars could reduce prescription drug costs by $44 billion over the next 10 years. So why is biosimilar adoption so low? A paper by Edgar et al. (2021) provides one rationale: the presence of prior authorization restrictions on biosimilars.
Another challenges occurs with physician-administered biologic/biosimilar medications due to financial incentives. Physicians can charge payers (e.g., Medicare) 106% of the average sales price (ASP) for products with the same billing code. As noted by a USC-Brookings paper, this system:
The Edgar paper continues on with some suggestions on how to overcome these barriers including educating providers and pharmacists, removing prior authorizations, reducing patient cost sharing for biosimilars, and potentially even increasing provider reimbursement for prescribing biosimilars. While biosimilar offer much promise for reducing cost, enacting steps to make it easier to prescribe biosimilars is imperative. Via Dental Tips http://www.rssmix.com/via Blogger http://jeanxrussell.blogspot.com/2021/09/barriers-to-biosimilar-adoption.html September 23, 2021 at 06:45AM
Healthcare Expert and Former Congresswoman Allyson Y. Schwartz Joins FTI Consulting as Senior Advisor
An exciting addition to the FTI team. Below is the press release:
I’m excited to collaborate with Congresswoman Schwartz connecting rigorous health economic analyses to address important policy issues. Via Dental Tips http://www.rssmix.com/via Blogger http://jeanxrussell.blogspot.com/2021/09/healthcare-expert-and-former.html September 22, 2021 at 12:45AM
What will be the impact of adopting reference pricing in the US?
That is the question that a recent JAMA study–Mulcahy et al. (2021)–aim to answer. The authors use IQVIA MIDAS data to estimate sales price and volume in the US. These can can be used to estimate drug wholesale acquisition cost (WAC), but they ignore rebates. To account for rebates in the US they use SSR Health information Then international prices are identified based on the IQVIA MIDAS data across 6 markets (Australia, Canada, France, Germany, Japan, and the U.K). The authors then calculate US wholesale prices, US net prices and what US prices would be if drugs were reference priced to these 6 markets. Based on this approach, they find that:
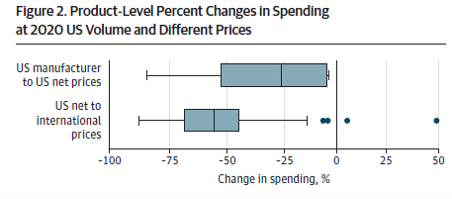
So if reference prices were enacted as proposed in H.R. 3, could we expect a 50% decrease in prices in the US? The answer is ‘no’. The reason for this is that the Mulcahy et al. paper examines the impact of reference prices in a static rather than a dynamic setting. As noted in a recent Commonwealth Report, pharmaceutical firms are likely to alter their pricing strategies if reference pricing were adopted in the U.S. They may not accept lower prices in reference-priced countries or may delay entry in these markets. The countries included in the reference basket may also respond as well. As the Commonwealth Fund report states:
Also, launch prices may be higher as well. Title II of H.R. 3 would impose rebates to offset prices that increase faster than inflation. To insure the net present value of a drug’s revenue of it’s lifetime remains similar, it is likely that pharmaceutical firms would pursue high launch prices, if prices are highly constrained over time. In short, reference pricing is likely to lead to lower prices in the U.S. (but not as much as expected by via Blogger http://jeanxrussell.blogspot.com/2021/09/what-will-be-impact-of-adopting.html September 21, 2021 at 11:45AM
Are patients able to shop for lower priced providers?
This is what a study by Whaley et al. (2021) aims to find out.
The authors use health insurance claims data for about 4 million individuals to find the answer. They examine changes in average price paid and provider market share for patients who’s employers introduced the new benefit design with patient direct payments compared to patients without this incentive.
One key concern if you pay patients would be whether individuals use health care services just to get paid to do so. Thus, while the scheme appears to have had its intended impact of lowering the prices employers paid, it is unclear the extent to which such a scheme could be rolled out more broadly. Further, for Medicare patients, balance billing is de facto prohibited thus making patient incentives for this patient population more difficult to implement. Via Dental Tips http://www.rssmix.com/via Blogger http://jeanxrussell.blogspot.com/2021/09/are-patients-able-to-shop-for-lower.html September 20, 2021 at 03:45AM |
 RSS Feed
RSS Feed
